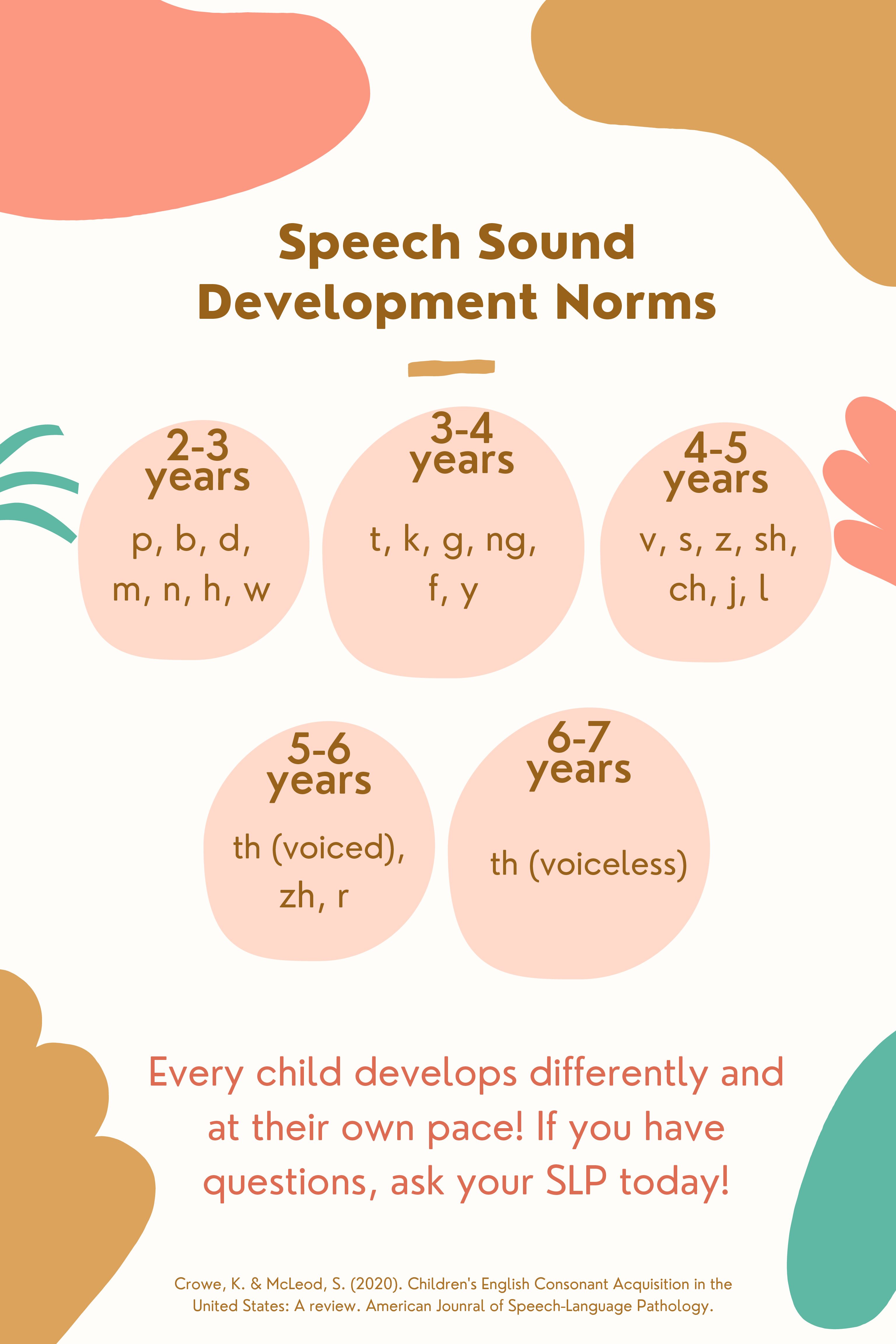
Speech sound development norms
0

Occupational therapy (OT) treatment focuses on helping people with a physical, sensory, or cognitive disability be as independent as possible in all areas of their lives. OT can help kids with various needs improve their cognitive, physical, sensory, and motor skills and enhance their self-esteem and sense of accomplishment.
Some people may think that occupational therapy is only for adults; kids, after all, do not have occupations. But a child’s main job is playing and learning, and occupational therapists can evaluate kids’ skills for playing, school performance, and daily activities and compare them with what is developmentally appropriate for that age group.
According to the American Occupational Therapy Association (AOTA), in addition to dealing with an someone’s physical well-being, OT practitioners address psychological, social, and environmental factors that can affect functioning in different ways. This approach makes OT a vital part of health care for some kids.


Technology has transformed the way both adults and children live. Screens have dramatically changed the world of children’s play. Nowadays, little ones spend more time watching television than playing outdoors. Children’s interaction with technology includes large variations such as watching television, playing digital games, using video chats or apps to communicate, or using digital tools to create content, etc. The question for us, as parents, educators, and pediatric professionals is what, how much, and at what pace should we introduce children to the various faces of electronic media.
How to find out what is developmentally appropriate for your little ones when it comes to technology?
Determining when and how to use various technology-based on Three C’S
David Elkind, author of “the power of play” explains media content as hot and cold depending upon the level of participation it can allow. For example- The sketch invites more participation than does a photograph. Now let’s consider several factors that make any content whether a computer game, TV program hot or cool. Additionally while considering what content is hot or cool for a specific child, every child would have varying responses and individual differences in their preference for hot and cool media.
Hot content |
Cool content |
· Less participation, decreased active learning opportunity · Stimulating, visually arresting, fast paced · Violent and entertaining TV shows · For e.g., For infants and young toddlers, TV shows utilizing attention getting strategies such as bright colors, high pitch sounds and liberal use of repetitive large movements. Infants would prefer to watch such hot media but more likely to be entertained than to engage in active learning |
· More participation, increased learning opportunity · Quiet, slow paced, visually interesting · Educational TV shows · For e.g., For infants and young toddler’s TV shows with less intrusive visuals, soothing music, scan be used by parents and caregivers during their normal routine activities like diaper change, getting dressed etc. |
The most imperative factor to be considered while understanding the importance of technology usage with young children is, the context in which the technology is used. It should help in increasing learning opportunities in children.
Passive and Active use of technology
Passive use of technology– It occurs when children are consuming content, such as watching a program on television, playing a game on a computer, without any active participation, accompanying reflection, imagination.
Active use of technology– It occurs when children use technologies such as computers, devices, and apps to engage in meaningful learning and active engagement. Examples include sharing their experiences by documenting them with photos and stories, recording their own music, using video chatting software to communicate with loved ones, or using an app to guide playing a physical game. These types of uses are capable of deeply engaging the child, especially when an adult supports them.
Examples of active use of technology
Families can promote the exchange of ideas and expand the child’s imagination by viewing various programs with young children and maximizing their learning opportunities. Most research on children’s media usage shows that children learn more from content when parents or early educators watch and interact with children, encouraging them to make real world connections to what they are viewing both while they are viewing and afterward.
Amid a global pandemic, the use of video-chat interactions has helped to promote relationships. Schools are virtual which gives an opportunity for children to connect and build positive peer relationship via video chats as well as with educators. While video chatting can be done at any age (as interactions tend to be brief and guided by an adult), new evidence shows that infants and toddlers can attend to and engage in joint attention during video-chat interactions but do so more effectively after approximately 16 months of age and with parental support.
Every child is unique and so would be their choices. Considering the fact that nothing can replace the face to face interactions and the benefits of natural play for children, there are specific recommendations put forward by American Pediatric Association for various age ranges from 0-8 years with regards to technology usage in children.
Under the age of 2 |
The American Academy of Pediatrics(AAP) has advised parents against television by children under two years of age. It can be used as a platform to support relationships such as video chatting with family members as a form of social interaction. Parents who are interested in using media with their children can start around 18 months with high-quality content but should always co-view content and use technology with their children. |
Ages 2-5 |
New recommendations in the American Association of Pediatrics AAP’s 2016 Media and Young Minds Brief suggest that one hour of technology use is appropriate per day, inclusive of time spent at home and in early learning settings and across devices |
Ages 6-8 |
Technology should be used as a tool for children at this age to explore and become active creators of content. If they are using virtual learning at school and have more than one teacher, those teachers should be aware of how much screen time is being used across subject areas and at home. Students should learn to use technology as an integrated part of a diverse curriculum. At home, parents should set limits they feel are appropriate for their children, understanding the differences between passive and active technology use as well as the benefits of using technology with an adult versus solo use. Parents should also be aware of how much technology is being used in the classroom, what is needed for homework, and how this fit into an overall picture of technology use for their child throughout the day. The AAP has created an interactive Family Media Plan Tool on HealthyChildren.org to help parents be thoughtful about media exposure for their children.
|

Parents are the initial evaluators to spot signs and symptoms of DCD in their child before anyone else. When they notice their little one is struggling, having challenges or lacking behind other children in movement skills, such as sitting up or learning to walk. However, sometimes signs and symptoms of DCD are not caught until a child starts school. Teachers may see that the child cannot play at recess or in physical education classes in the same way that other children do. They also may observe that it takes the child longer to complete schoolwork. Children with DCD show a lack of interest in playing with other children.
Children with DCD may have difficulty when they try to:
Preschool Has trouble throwing a ball Plays too roughly or often bump into other kids by accident Has difficulty sitting upright or still Grade K-2 Has trouble holding and using a crayon, a pencil, or scissors Doesn’t form or space letters correctly Struggles with going up and downstairs Frequently bumps into people by accident Has trouble with self-care, like brushing teeth Grade 3-7 Takes a long time to write Has trouble cutting foods Has difficulty with basic routines like getting dressed Struggles to line up columns when doing math problems
Historically, parents have been told not to worry about their child’s clumsiness because the child will outgrow the problem. However, current researchers in the area of DCD report that the children do not outgrow clumsiness and that, without intervention, they will not improve. A key treatment for DCD is occupational therapy (OT). There are many examples of how occupational therapists can work on challenging motor tasks. They might have kids trace letters on sandpaper to build handwriting skills, for example. Or use a lacing board with different colored laces to practice shoe tying. Kids with DCD may also work with physical therapists on balance and muscle tone. Occupational therapy and Physical Therapy assist with helping the child with DCD develop movement strategies that increase coordination, motor planning, balance, strength and body awareness resulting in a decrease in overall clumsiness and increased ability to perform functional activities at home, school and in the community. Speech and language therapy may also be required to help the child with the oral motor skills required for swallowing, chewing and speech.
References
Harrowell, I., Hollén, L., Lingam, R., & Emond, A. (2018). The impact of developmental coordination disorder on educational achievement in secondary school. Research in developmental disabilities, 72, 13-22.
Kirby, A., & Sugden, D. A. (2007). Children with developmental coordination disorders. Journal of the royal society of medicine, 100(4), 182-186.
https://www.understood.org/en/learning-thinking-differences/child-learning-disabilities/dyspraxia/understanding-developmental-coordination-disorder-dcd

When one sound is substituted by another sound in a systematic fashion
| Phonological Process | Definition | Age | Example |
|---|---|---|---|
| Affrication | Fricatives are replaced by affricates | 3;0 (Peña-Brooks & Hedge, 2007) |
[dɔr] -> [jɔr] |
| Alveolarization | Non alveolar sound is replaced with an alveolar sound | 5;0 (Peña-Brooks & Hedge, 2007) |
[ʃu] -> [tu] |
| Backing | Sounds are substituted or replaced by segments produced posterior to , or further back in, the oral cavity than the standard production | No information available | [sɪp] ->[ʃɪp] |
| Deaffrication | Affricates are realized as fricatives | 4;0 (Peña-Brooks & Hedge, 2007) |
[tʃɪp] -> [ʃɪp] |
| Depalatization | Palatal sounds are realized as sounds produced further forward in the oral cavity | 5;0 | [fɪʃ] -> [fɪt] |
| Fronting | Velars are realized as sounds produced further forward in the oral cavity | 3;6 (Bowen,1998) |
[go] -> [do] |
| Gliding of liquids | Liquids /l,r/ are replaced by a glide /w,j/ or another liquid | 5;0 (Bowen,1998) |
[lif] -> [wif] |
| Labialization | Nonlabial sound is replaced with a labial sound | 6;0 (Peña-Brooks & Hedge, 2007) |
[taɪ] -> [paɪ] |
| Stopping | Fricatives and/or affricates are realized as stops | 5;0 (Bowen,1998) |
[piʧ] -> [pit] |
| Vocalization | Liquids or nasals are replaced by vowels | /f/&/s/ =3;0 /v/ & /z/ =3;6 /ʃ/,/tʃ/,/j/=4;6 (Bowen,1998) |
[teɪbəl] -> [tebo] |
| Denasalization | Nasals are replaced by homorganic stops | 2;6 (Peña-Brooks & Hedge, 2007) |
[naɪs] -> [daɪs] |
| Glottal replacement | Glottal stops replace sounds usually in either intervocalic or final position | No information available | Tooth-> |
| Prevocalic voicing | Voiceless consonants in the prevocalic position are voiced | 3;0 (Bowen,1998) |
[teɪbəl] -> [debi] |
| Devoicing of final consonants | Voiced obstruents are devoiced in final position | 3;0 (Bowen,1998) |
[dɔg] -> [dɔk] |
[/bt_text][bt_text]
When one sound in the word becomes similar to another sound in the word
| Phonological Process | Definition | Age | Example |
|---|---|---|---|
| Assimilation (consonant harmony) | One sound is replaced by another that is the same or similar to another sound within the word | 3;0 (Peña-Brooks & Hedge, 2007) |
[dɔg] ->[dɔd] |
| Velar Assimilation | A nonvelar sound is assimilated to a velar sound because of the influence, or dominance, of a velar |
3;0 (Peña-Brooks & Hedge, 2007) |
[dʌk] -> [gʌk] |
| Nasal Assimilation | A non-nasal sound is assimilated and replaced by a nasal because of the influence, or dominance, of a nasal consonant | 3;0 (Peña-Brooks & Hedge, 2007) |
[læm] -> [næm] |
| Labial Assimilation | A nonlabial sound is assimilated to a labial consonant because of the influence of a labial consonant. | 3;0 (Peña-Brooks & Hedge, 2007) |
[bɛd] -> [bɛb] |
| Alveolar Assimilation | Non-alveolar sound is changed to an alveolar sound | 3;0 (Peña-Brooks & Hedge, 2007) |
[tos] -> [tot] |
[/bt_text][bt_text]
Phonological processes that affect the syllable structure
Phonological
| Phonological Process | Definition | Age | Example |
|---|---|---|---|
| Consonant Cluster Reduction | Deletion of one element of the cluster | 4;0 (Bowen,1998) |
[stɑp] -> [tɑp] |
| Epenthesis | A segment, often the unstressed vowel, is inserted | 8 (Peña-Brooks & Hedge, 2007) |
[blæk] ->[ bəlæk] |
| Reduplication | A syllable or a portion of a syllable is repeated or duplicated, usually becoming CVCV | 3;0 (Bowen,1998) |
[dæd] -> [dæ dæ] |
| Weak/Unstressed Syllable Deletion | Deletion of the unstressed syllable | 4;0 (Bowen,1998) |
[tɛləfon] -> [tɛfon] |
| Final Consonant Deletion | Deletion of the final consonant in the word | 3;3 (open and closed) (Bowen,1998) |
[kæp] ->[ kæ] |
| Consonant Cluster Simplification | A consonant cluster is simplified by a substitution for one member of the cluster | 4;0 (Bowen,1998) |
[ski]->[sti] |
| Metathesis | There is a transposition or reversal of two segments (sounds) in a word | No information available | [bæskət] -> [bæksɪt] |
| Coalescence | Characteristics of features from two adjacent sounds are combined so that one sound replaces two other sounds | No information available | [swɪm] ->[ fɪm] |
[/bt_text][/bt_column][/bt_row][/bt_section]

| Hearing and Understanding | Talking |
|---|---|
Birth-3 Months
|
Birth-3 Months
|
4-6 Months
|
4-6 Months
|
7 Months-1 Year
|
7 Months-1 Year • Babbling has both long and short groups of sounds such as “tata upup bibibibi.”
|
One to Two Years
|
One to Two Years
|
Two to Three Years
|
Two to Three Years
|
Three to Four Years
|
Three to Four Years
|
Four to Five Years
|
Four to Five Years
|
[/bt_text][/bt_column][/bt_row][/bt_section]
Note: “bilingual” refers to someone who speaks two languages; “monolingual” refers to someone who speaks one language
The Facts: What We Know About Bilingualism
Our world is becoming increasingly multilingual. Consider some of the following statistics:
In Canada….
In the United States….
Worldwide, it is estimated that….
These trends mean that many children are being raised as bilinguals. Sometimes bilingualism is a necessity, as a child’s parents may not be fluent in the majority (dominant) language spoken in the community. Therefore, the child may learn one language at home and another at school. But sometimes bilingualism is a choice, and parents may wish to expose their child to another language, even if they do not speak a second language themselves. This could be due to the many benefits of being bilingual.
The cognitive advantages of bilingualism (e.g . with attention, problem solving, etc.) seem to be related
to an individual’s proficiency in his languages (10). This means that a person will benefit more from his
bilingualism (cognitively) if he is more proficient in his languages.
Bilingual acquisition can take place in one of two ways:
A child who acquires a second language in this manner generally experiences the following (10):
|
FALSE. While a bilingual child’s vocabulary in each individual language may be smaller than average, his total vocabulary (from both languages) will be at least the same size as a monolingual child (10, 15). Bilingual children may say their first words slightly later than monolingual children, but still within the normal age range (between 8-15 months) (11). And when bilingual children start to produce short sentences, they develop grammar along the same patterns and timelines as children learning one language (5). Bilingualism itself does not cause language delay (10). A bilingual child who is demonstrating significant delays in language milestones could have a language disorder and should be seen by a speech language pathologist.
FALSE. When children use both languages within the same sentence or conversation, it is known as “code mixing” or “code switching”. Examples of English-French code-mixing: “big bobo” (“bruise” or “cut”), or “je veux aller manger tomato” (“I want to go eat..”) (10). Parents sometimes worry that this mixing is a sign of language delay or confusion. However, code mixing is a natural part of bilingualism (17). Proficient adult bilinguals code mix when they converse with other bilinguals, and it should be expected that bilingual children will code-mix when speaking with other bilinguals (5).
Many researchers see code mixing as a sign of bilingual proficiency. For example, bilingual children adjust the amount of code-mixing they use to match that of a new conversational partner (someone they’ve never met before who also code mixes) (5). It has also been suggested that children code-mix when they know a word in one language but not the other (13). Furthermore, sometimes code-mixing is used to emphasize something, express emotion, or to highlight what someone else said in the other language. For example, “Y luego él dijo STOP” (Spanish mixed with English: “And then he said STOP!”) (10). Therefore, code-mixing is natural and should be expected in bilingual children.
FALSE. It is rare to find an individual who is equally proficient in both languages (16). Most bilinguals have a “dominant language”, a language of greater proficiency. The dominant language is often influenced by the majority language of the society in which the individual lives (6). An individual’s dominant language can change with age, circumstance, education, social network, employment, and many other factors (16).
FALSE. There is a “Critical Period” theory that suggests that there is a window of time (early childhood) during which a second language is most easily learned. This theory has led many people to believe that it is better to learn a second language as a young child. Young children have been found to achieve better native-like pronunciation than older children or adult second language learners. And they seem to achieve better long-term grammatical skills than older learners (10). But other findings have called the idea of a critical period into question. For example:
Therefore, while younger children seem to become more “native-like” in the long-term, older children may pick up vocabulary, grammar, and academic language more easily in the initial stages of language learning.
FALSE. Some parents may choose to adopt the “one parent-one language” approach, where each parent speaks a different language to the child. While this is one option for raising a bilingual child, there is no evidence to suggest that it is the only or best way to raise a child bilingually, or that it reduces code mixing (10). Parents should not worry if they both speak their native language to the child or if they mix languages with their child (19), as it has been recognized that children will mix their languages regardless of the parents’ approach (10). Many approaches can lead to bilingualism. Parents should speak to their child in a way that is comfortable and natural to them.
FALSE. Some parents attempt to speak the majority language to their child because they want their child to learn that language, even if they themselves are not fluent in the majority language. This can mean that conversations and interactions do not feel natural or comfortable between parent and child. There is no evidence that frequent use of the second language in the home is essential for a child to learn a second language (10). Furthermore, without knowledge of a family’s home language, a child can become isolated from family members who only speak the home language. Research shows that children who have a strong foundation in their home language more easily learn a second language. Children are also at great risk of losing their home language if it is not supported continually at home.
There are many ways to support your child’s bilingualism:

You may have seen someone write in a notebook to answer a question. Maybe you have seen people using sign language or other gestures. You may have seen someone push buttons on a computer that speaks for them. These are all forms of augmentative and alternative communication, or AAC.
AAC includes all of the ways we share our ideas and feelings without talking. We all use forms of AAC every day. You use AAC when you use facial expressions or gestures instead of talking. You use AAC when you write a note and pass it to a friend or coworker. We may not realize how often we communicate without talking.
People with severe speech or language problems may need AAC to help them communicate. Some may use it all of the time. Others may say some words but use AAC for longer sentences or with people they don’t know well. AAC can help in school, at work, and when talking with friends and family.
Do you or your loved one have difficulty talking? There are options that might help. There are two main types of AAC—unaided systems and aided systems. You may use one or both types. Most people who use AAC use a combination of AAC types to communicate.
You do not need anything but your own body to use unaided systems. These include gestures, body language, facial expressions, and sign language.
An aided system uses some sort of tool or device. There are two types of aided systems—basic and high-tech. A pen and paper is a basic aided system. Pointing to letters, words, or pictures on a board is a basic aided system. Touching letters or pictures on a computer screen that speaks for you is a high-tech aided system. Some of these speech-generating devices, or SGDs, can speak in different languages.
An SLP will test how well you or your loved one can speak and understand. The SLP can help find the right AAC system for you. You may use a basic system first and may need it for only a short time. This may happen if you had mouth surgery or a stroke and your speech comes back.
It may take some time to get a more high-tech system, if you need one. Not every device works for every person, so it is important to find the right one for you. The Information for AAC Users webpage has more information about finding the best AAC system. Insurance or other funding can help you pay for your AAC device.
See ASHA information for professionals on the Practice Portal’s Augmentative and Alternative Communication page.

The ability to hear is essential for proper speech and language development. Hearing problems may be suspected in children who are not responding to sounds or who are not developing their language skills appropriately. The following are some age-related guidelines that may help to decide if your child is experiencing hearing problems.
It is important to remember that not every child is the same. Children reach milestones at different ages. Talk your child’s healthcare provider if you are suspicious that your child is not developing speech and language skills correctly. The National Institute on Deafness and Other Communication Disorders and other experts list the following age-appropriate speech and language milestones for babies and young children.
| Birth to 5 months |
|
|---|---|
| 6 to 11 months |
|
| 12 to 17 months |
|
| 18 to 23 months |
|
| 2 to 3 years |
|
| 3 to 4 years |
|
| 4 to 5 years |
|
| 5 years |
|
Children grow and develop at their own rate. Although some children walk and talk early, others may be delayed in learning certain skills. If you have any concerns about your child’s development, the earlier you seek help, the better.
Early intervention is for children ages birth to 3 and their families. Early intervention is available in every state under federal law. In some states, early intervention programs may continue until a child is age 5.
Families and professionals, including audiologists and speech-language pathologists, are part of an early intervention team. They help children develop skills such as
Early intervention is different for each child and family depending on the child’s needs and the family’s priorities. The most important step is to start early.
Health care providers, parents, child care staff, teachers, and social service workers are just some of the people who can refer an infant or toddler for early intervention.
If you are concerned about your child’s development, you may contact your local early intervention program directly to ask for an evaluation. Families do not have to wait for a referral from professionals.
You can find your community’s early intervention office by
After your child is referred to your local early intervention program, a service coordinator will meet with you and your child to gather information and explain next steps. They will evaluate your child’s skills to see if your child and family are eligible for services. They will ask you for written consent before they begin.
If your child is eligible for services, a more in-depth assessment (i.e., tests, observations, interviews) will be completed. This assessment determines how early intervention can help your child and family.
Next, the early intervention team writes an Individualized Family Service Plan. This plan includes goals, services, and supports for your child and family. You are part of the team, and you help decide what is included in the plan.
Early intervention services must be in the language(s) your child and your family use. If necessary, an interpreter will work with you and the early intervention providers.
A few months before your child’s third birthday, you and the early intervention team will develop a transition plan to meet the needs of your child and family. Part of this plan involves deciding if your child needs services after age 3.
Some states will extend early intervention services beyond your child’s third birthday if needed. Children older than 3 may be eligible for services from the local school district.
If your child does not qualify for services, but you feel they still need help, let the team know right away. You can request another evaluation at that time or in the future. You can also seek services outside of the early intervention program. These services are usually billed to you or your insurance.
If your child is already 3, you can still get help through your local school district. Each school district has a program called Child Find that can help.
A lot happens in the first few years of life. For children who are not where they need to be with development, getting help early can make a big difference.
See these ASHA resources for more information about typical development and early signs of speech, language, and hearing disorders:
You can also browse ASHA’s Online Store for brochures and booklets related to infants and toddlers.